
Asthma ICD 10
Regarding the new coding system ICD-10, it can be considered completely implemented. There are some of the codes that seem improbable or incompetent.
The new coding system, according to the information from the primary care providers, ICD-10 takes too much time and is frustrating, as it takes time from the patient care. Changing the code system is a very time-consuming process. It’s a long process, firstly concerning a patient suffering from asthma, although the changes in asthma codes have been particularly far-reaching.
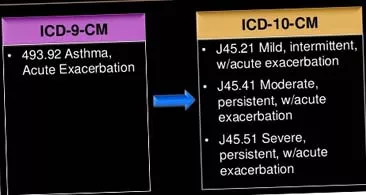
The new code system for asthma ICD-10 can be thought to be too complicated, but it has its advantages and benefits. The ICD-9 asthma codes, previously used, were based on the doctor’s ability to determine which asthma form a patient had: an external (allergic) asthma or an internal asthma (asthma, caused by strokes or some irritants). This data is not available to most suppliers. The supplier can only know this information if the patient has previously been tested for a skin allergy or had a RAST serum testing. According to the requirements of the new code system ICD-10, the doctor must classify the type of the patient’s asthma, according to different levels of seriousness.
A huge number of people seek emergency medical care because of asthma attacks. There are a lot of reasons for inadequate asthma control, which can even lead to the patient's death. They are associated with the use of patient’s plans of actions for asthma, also with the patient’s receiving appropriate drugs and the doctor’s disease monitoring. According to some data, there are drawbacks in primary care of patients. A lot of mistakes are made in observing asthma instructions by patients.
It's quite easy to classify the asthma severity. The new ICD-10 coding system will help the suppliers to determine the asthma, even meeting a patient for the first time. Sometimes it happens that the patients themselves do not know about their disease severity. Most patients take drugs that are prescription-dispensed and, in this case, it is difficult to monitor them.
Spreading asthma medicines, the providers should ask the patients about the symptoms they have and the symptoms frequency, they should ask about the ways the patients use their inhalers and how often they do it. This should all be done in order to classify the asthma severity and to conduct the control, also to be sure that the patients receive all the right medications and know how to take them in a right way. If a patient needs using a rescue inhaler daily, then the severity of his asthma will be identified as either severe or moderate. Within the patients with a severe or moderate asthma severity, the pharmaceutical regimen of daily inhalations or a combined therapy should be minimal. In the case, when the classification of asthma control does not match the patient's prescription therapy, the treatment options should be reviewed.
For some disease models, the new ICD-10 coding system may seem unacceptable, but in the case of asthma treatment, the necessary changes can be beneficial. If the providers start to study this problem better and produce more control over asthma, then the prescription therapy will become more appropriate.
Asking the patients about the way they use their inhalers and how often they do it takes a little time and it will be not difficult to determine their level of asthma control. This can lead to better patient outcomes, reduced seeking medical care and healthier patients.